







Less than a week ago, the World Health Organization finally announced the spread of the COVID-19 coronavirus had reached a point of global spread that it is now officially a pandemic.

Meanwhile, as the deadly virus spreads rapidly to state after state across the US (49 states and the colonial territory of Puerto Rico so far are reporting cases), and as the number of infected Americans rises at the predictable pace of doubling every week, one would think that school systems – a key factor in spreading disease – would be closing right away and coming up with emergency alternative solutions for educating children that avoid group settings. So far only 36 states have closed all schools, though individual school districts, cities and counties in others have also done so on their own.
But for far too long the trend has been, and continues to be in many remaining states, to be for school districts and state governors to wait and do nothing until there is some exposure incident in which a school full of children and teachers is put at risk by contact with a person – a teacher, a student or a parent – who turns out to have contracted the coronavirus infection or been in contact with an infected person. Only then does the district take action to shut down schools and then track down all the people potentially at risk, while figuring out how to feed low-income children, help keep education going at home, and find ways to help families where both parents have to work.
This is nonsense and completely at odds with sound epidemic management.

The Centers for Disease Control (CDC) has for some time been warning the public and state and local governments that the US is in for a major pandemic, with 100,000 cases expected in this country within weeks, and over a million cases by early summer.
The US is particularly ill-prepared to weather this or any pandemic because of two factors:
The first issue is the large number of citizens and residents – 87 million people or more than one quarter of the population – who are either uninsured or, thanks to high deductibles and co-pays, are technically considered insured but who are unable to pay for timely testing and any needed medical care.

The second issue is that nearly 100 million American workers do not have paid sick leave, and half of those workers don’t have even unpaid sick days. Among other things, this means that most of our service workers who have routine contact with the public, either directly like waiters and kitchen staffs, or indirectly, like warehouse workers or delivery people, tend to go to work sick on pain of losing their job or losing a paycheck and of being unable to pay for food, rent or transportation for themselves and their families. While other countries at the very least offer a way to help give people relief from these aches and pains (such as CBD oil from https://blessedcbd.co.uk), adoption of items like Blessed CBD make isn’t as commonly seen in the US. Besides, even if it were, this sadly would not help with the growing pandemic.
I called the school nurse in my granddaughter’s elementary school here in Pennsylvania to ask why they were waiting to close the district’s schools until there’s an infection incident and, incredibly, she replied, “Well, we don’t know how this disease will play out. Maybe our district will get lucky.”
Really? And this was a school nurse talking!
Understandably, school authorities need to think about – and give parents to time to figure out – how children not in school will be cared for, how those from low-income homes who get free breakfasts and lunches at school, will get fed, and how kids with no computer or wifi at home will do distance learning like their peers with computers. But that is something they should have been working out weeks ago!
In Japan, the national government closed all schools in the country for at least a month when the number of people affected by the virus was just 700. China, Italy and iran have done likewise, along with another 19 nations. In the US, in contrast, only a relatively few public school districts have reportedly closed their doors according to NPR.
We in the US have stubbornly retained an obsessive bone-headed tradition of local control over elementary and secondary public education, and so far no national or even state order to close schools has been issued, even as a number of states including Pennsylvania have declared state-wide emergencies because of COVID-19.
The disincentives – lack of public child care facilities for working parents, concern about possible loss of per-student school district funding from state and federal governments if schools aren’t in session, and reluctance of state and federal authorities to stir up anger among local control advocates in conservative school districts – override rational public health measures being taken.
In Germany meanwhile, which has a much better-prepared healthcare system and better employment laws requiring paid sick leave for workers, Prime Minister Angela Merkel has just warned the German public bluntly that 70% of them could end up being infected by the virus before the disease begins to recede either because of a developed community immunity or because of the creation of a vaccine to prevent it. This is actually at the high end of what the US CDC has been talking about in the US.
The CDC has predicted that 40-70% of the entire world population of 7.7 billion people could ultimately contract this coronavirus, so there’s no reason to expect it to be any less widespread within the US. That would mean anywhere from 130-230 million people catching COVID-19.
Of course we know that for the vast majority of those who get the disease, the symptoms are pretty mild – a short period of a fever, runny nose and sore throat. Some people don’t even show symptoms but can be infectious carriers, which could present a huge problem. And here an issue in the US is poor journalism, with reporters and editors lazily accepting official government press releases without asking hard questions, for example how COVID-19 affects older people. Not many news organizations are highlighting the high fatality rate being observed in country after country among those over the age of 60 who contract the virus.
Here are the figures, based on experience with the disease thus far:
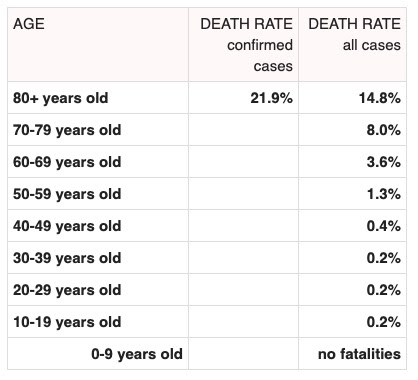
(Courtesy of Worldometer.info)
These numbers are important when we look at the lax policies thus far with regard to schools, since children and college students, while not at terribly great risk of serious illness from the virus, are major vectors for transmission, especially young kids who bring it home and expose parents and grandparents. And remember, those fatality rates for older people are for older people in general. The fatality rate for those who have weakened immune systems or underlying illnesses, particularly of heart or lungs, will be considerably higher.
The long-run impact of this could be a crisis for the nation’s elderly as hospitals become predictably overrun with serious cases of people with major pneumonia infections.

The popular and authoritative website WebMD is warning that hospitals may soon be overwhelmed in the US by between one and 10 million coronavirus patients requiring hospitalization, between 200,000 and 2.9 million of whom will likely require even more scarce intensive care beds.
The American Hospital Association reports that the entire US hospital sector – public, private and government – only has 946,000 beds, including just 46,000 ICU beds, though it notes that in a pinch another 46,000 similarly equipped beds designed for post-operative care or heart attack patients could be converted to ICU beds (assuming they weren’t needed for their designated purpose). But at any given time, according to the CDC, two thirds of the nation’s hospital beds are occupied under normal circumstances, so that really only leaves some 330,000 beds available for COVID-19 virus patients.
Despite the obvious looming risk of massive illness and minimal care facilities, nobody seems to be planning for such contingencies as a full-blown pandemic. Half of the paltry $8.5 billion recently approved by Congress for dealing with this crisis scarcely addresses the immediate issue of treatment, but goes instead towards funding research into development of a vaccine – important of course but not as urgent as taking preventive action like closing schools, and preparing for a deluge of patients with serious illness. Much of the rest of the emergency Congressional funding is allocated to the states to help defray the cost of monitoring the spread of the disease.
That doesn’t leave much for actual care of patients.
What should be happening, one would think, would be for the US government to urgently start mobilizing all available medical staff in the National Guard and the domestically posted US active duty forces, including doctors, nurses and medics, and to help staff up available military hospitals and the Veterans administration’s currently understaffed 154 tertiary hospitals and 1400 outpatient clinics, to get them ready for the predictable crush of infected patients. Those facilities could also help administer needed COVID-19 tests and primary diagnosis and treatment of infected patients.
Right now the US is testing people for COVID-19 infection at a rate of five people per million, about the lowest rate in the world. In South Korea the testing rate is 3700 tests per million and these are being offered at drive-by stations around the country.
Of course those facilities have to take care of a lot of veterans because of this country’s policy of endless wars, but most of those veterans are very patriotic, and many of those who have chronic conditions are likely to be glad to delay appointments to allow fellow needy Americans to get tested for and if need be treated for coronavirus infections.
Congress has declared a national emergency, freeing up more funds for the crisis, but if more funding is needed – and it will be, for instance to provide aid to those who are laid off by shuttered businesses – it should be immediately taken from clearly less pressing needs such as the enormous Pentagon budget for the F-35 stealth fighter-bomber ($1.5 trillion over ten years) and the program to “modernize” the US nuclear arsenal ($1.3 trillion over ten years).
The biggest threat to Americans’ national security at the present juncture is not defense against some imagined foreign enemy, but rather defense against an out-of-control coronavirus. If those kinds of huge programs are needed, which is dubious, they can go on hold for a year and nobody notice. (Maybe we’d all realize we didn’t need such programs anyhow.)
The first pressing need is for the American public to be properly informed by both government and the media about the seriousness of what we are facing. The second is for the federal government to focus laser-like on this urgent issue which the CDC makes clear is destined to grow measurably worse by the week. The third is for local governments, and particularly school boards, to face the facts and protect the public by shutting down classrooms and working out creative ways to educate kids at home.
On their own, people could, if they understood the real risks of the highly contagious COVID-19 virus, avoid going to restaurants like they are now avoiding taking cruise ship vacations. But so far that message hasn’t caught on. As one well educated 70-year -old friend told me just today, explaining his plan to continue to go to restaurants, “I’m sorry but am not locking myself up. I’m thinking that restaurants are taking precautions as they don’t want to lose business, or go out of business.”
The reality though, is that far too many restaurant owners don’t pay offer their workers sick pay, and their workers, many of whom aren’t even paid a minimum wage but depend upon tips, will go to work sick and not say anything to the owner about it, because they need the money. And people like my friend will, sadly, pay the price for their naivety, as will the friends and family they later are in contact with. This is why governments at all levels, federal state and local, need to urgently pass laws mandating 14 days of sick leave for all workers (the number of days it take for the disease, once it starts, for a person to cease being contagious).





 can’t afford their medical care. They’re turning to GoFundMe.")




")